Clinical History : 28 years
female with severe back pain from 10 days.
H/O normal delivery 1 month back.
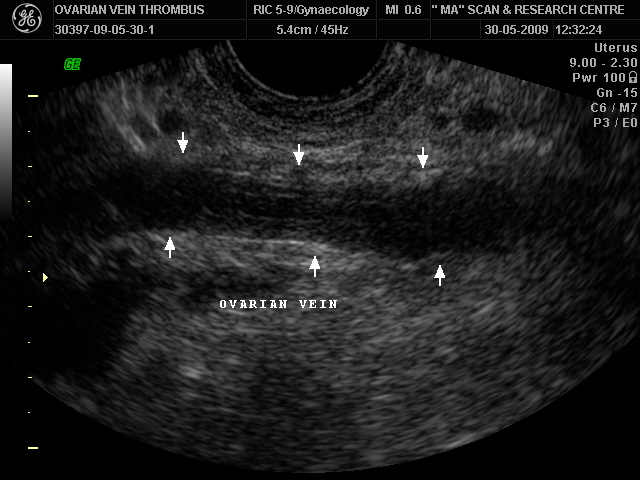
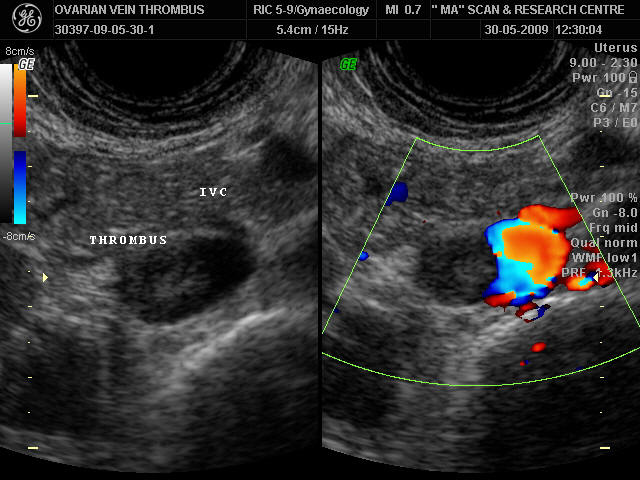
Ultrasound Findings :
Enlarged Rt. ovarian vein
filled with hypo echoic thrombus extending into IVC. On color
Doppler no E/o color uptake in the ovarian vein. Filling defect
noted in the IVC. Minimal free fluid noted in the pelvis.
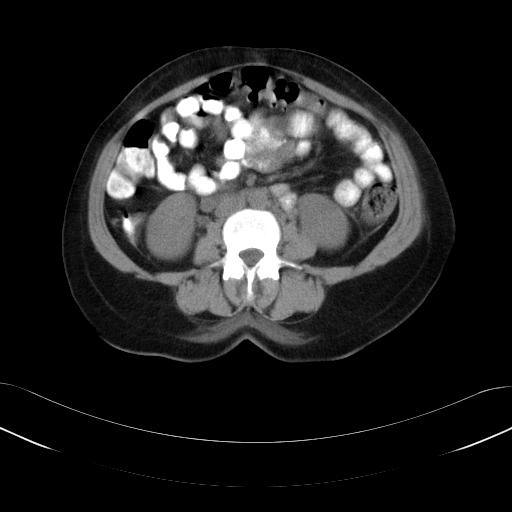
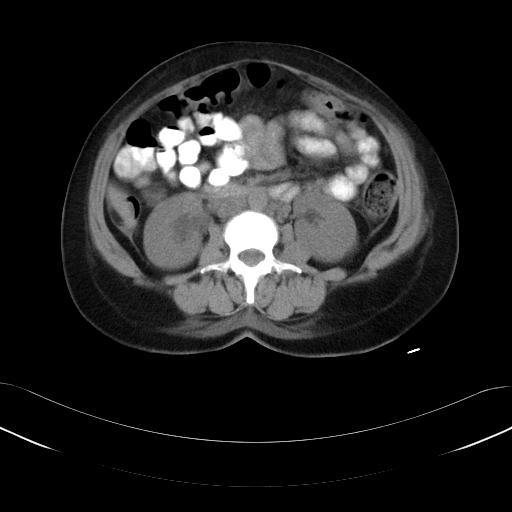
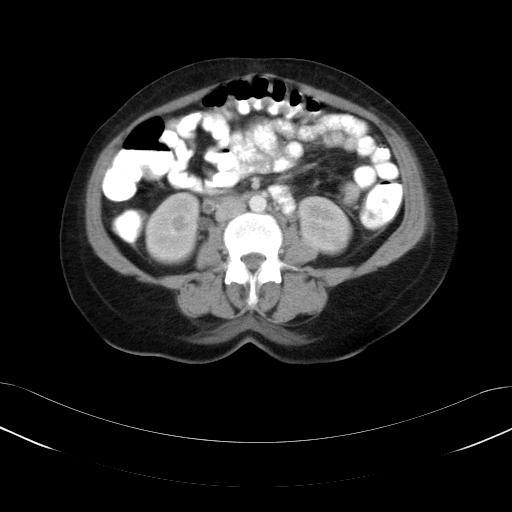
CT Scan findings:
Enlarged Rt. ovarian vein on
contrast showing peripheral wall enhancement with central non
enhancing area. Thrombus extending into the IVC.
Diagnosis : Rt.Ovarian vein
thrombosis.
Discussion
:
Introduction
The impact of ovarian
vein thrombosis and potential embolism on the postpartum patient
is significant. The incidence of pulmonary embolism in women
with postpartum ovarian vein thrombosis has been reported to be
from 13% to 33%. The thrombus may extend into the renal veins
and the IVC.
Incidence :
1:600 - 1:2000
deliveries 80% Rt. ovarian vein, 14% bilateral, 6% Lt. ovarian
vein
Etiology :
Puerperal ovarian
vein thrombophlebitis
Pelvic inflammatory
disease
Gynecologic surgery
Malignant tumors
Chemotherapy.
PATHOPHYSIOLOGY
The ovarian veins
arise from venules draining the ovaries, the broad ligament, and
the infundibulopelvic brim. The right ovarian vein usually
enters the anterolateral IVC at the L2 level, and the left
ovarian vein usually enters the left renal vein. Both vessels
are long and unbranched, and have incompetent valves.
During pregnancy, the
ovarian vein diameters increase 3-fold, flow capacity becomes 60
times greater, and valvular incompetence is exacerbated.
After childbirth,
blood flow in the ovarian veins immediately decreases, leading
to venous collapse and stasis . Altered coagulation is usual
after pregnancy. Hypercoagulability is present for 6 weeks
postpartum, caused by increased production of coagulation
factors 1, 2, 7, 10, and 11 and an increase in platelet
adhesiveness. These changes usually peak on the 4th postpartum
day.
CLINICAL FEATURES:
Symptoms typically
have an abrupt onset and include chills, fever, and lower
abdominal / flank pain. Palpable ropelike tender abdominal mass.
Thrombosis has been most frequently identified in the right
ovarian vein and is associated with RLQ pain. The right-sided
prevalence is due to the physiologic dextrorotation of the
uterus during pregnancy, which may compress the ovarian vein on
that side, and also to the direction of postpartum blood flow,
which is antegrade in the right ovarian vein and retrograde in
the left ovarian vein.
CT Scan Findings :
Tublar structure in
location of ovarian vein with low density center + peripheral
enhancement.
D.D
Endometritis, Acute
appendicitis, Hydronephrosis, Urolithiasis, Torsion of ovarian
cyst, Pelvic / Abdominal abscess or Pyelonephritis.
Reference :
5th Edition Radiology revew manual & Internet.
Submitted by: Dr.M.Adinarayana Rao,
MD.,RD.
Dr.
D.Prasada Reddy, DMRD.
Dr.G.Gowri Sekhar, DMRD., DNB.