|
|
|
| ||||||||||||||||||||||
|
Teaching File Series |
Last
|
| ||||||||||||||||||||||
|
M R I - Division | ||||||||||||||||||||||||
| Click on the images to view them closely | ||||||||||||||||||||||||
| ||||||||||||||||||||||||
| ||||||||||||||||||||||||
|
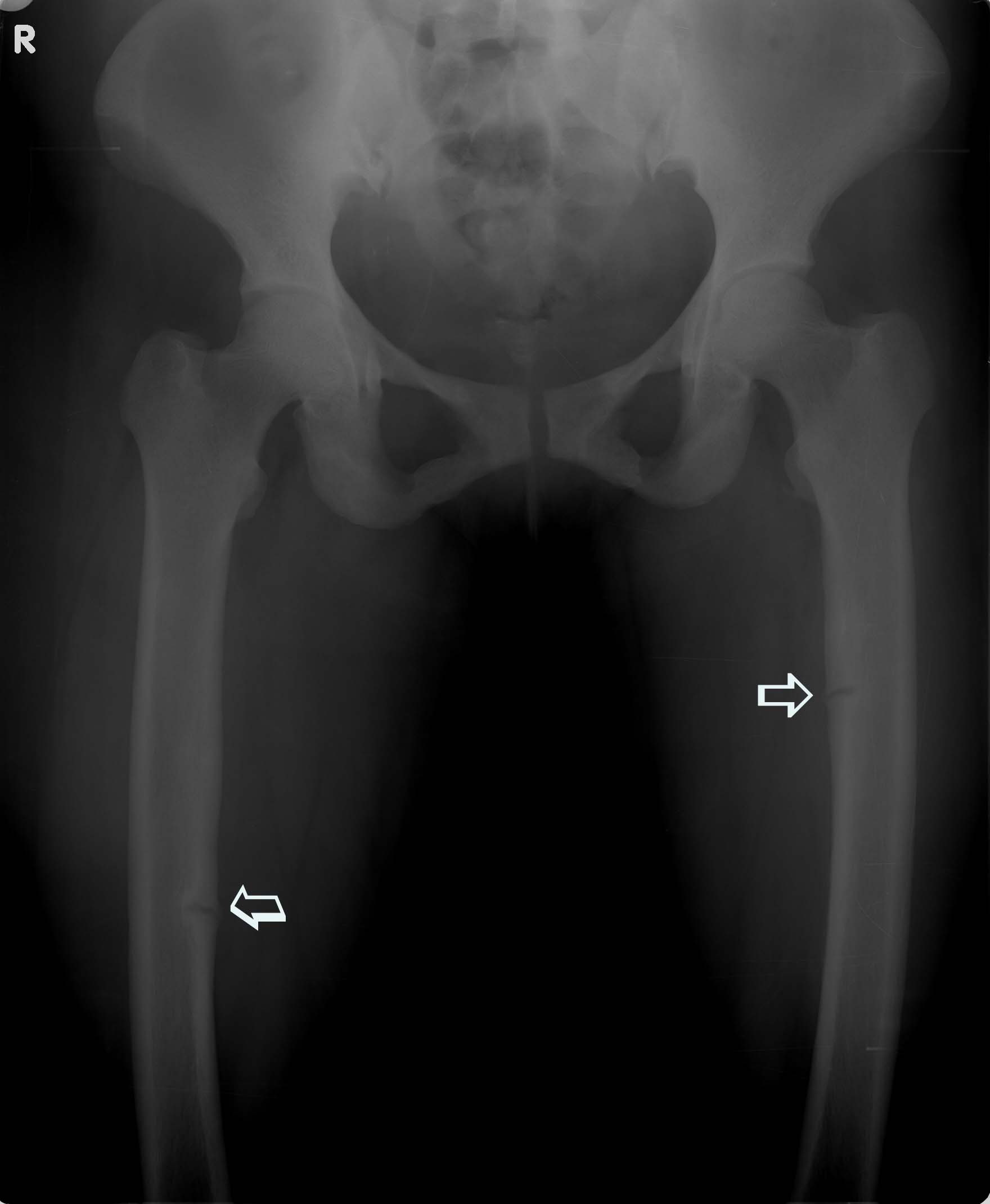
Complaint : 38Y, Non athletic female Right leg pain from one year. Investigation: X-ray AP View, CT Axial sections, MRI thigh, T1,T2 Wt. images of Coronal sections.
Two small incomplete transverse fractures (Arrows) with callus confined to medial cortex in the proximal &mid diaphysis of the femor, bilaterally. No E/o associated edema / soft tissue. Bone density is normal.
DISCUSSION : Bilateral femoral stress fractures are extremely uncommon, majority occur in athletes. Femoral stress fractures can be divided into those involving the femoral neck, condyles or shaft. Those of the femoral shaft are reported to comprise between 2.8 and 21 percent of femoral stress fractures in athletes.
Stress fractures occurred in both femurs, localized to both posteromedial shafts. This area of the femur has been shown to have the greatest strain in the sagittal plane, but is also susceptible to stress fracture due to the origin of the vastus medialis and the insertion of the adductor brevis.
In cases of overuse and elevated bone stress, it is suspected that either muscle fatigue leads to a decrease in the ability to absorb shock, and /or highly concentrated forces act through small areas of tendinous insertion to overload bone.
Femoral shaft stress fractures are stable stress fractures that can be treated with a progressive rehabilitation program.
REFERENCE : http://www.uihealthcare.com/depts/med/orthopaedicsurgery/research/ioj/ioj2005/sports/rarebilateral.pdf SUBMITTED BY: Academic division, 'MA' Advanced Diagnostic & Research Centre, Guntur, AP. INDIA. DR. M.ADINARAYANA RAO. MD. DR. G.GOWRI SEKHAR . DNB.,DMRD. DR. D. PRASAD REDDY. DMRD. DR.J.V.NARASIMHA RAO, MS.(ORTHO).
| ||||||||||||||||||||||||