|
Complaint : 40Y,
Female c/o
Headache from 3 months & visual disturbance from 1
week.
Investigation:
MRI Brain T1 & T2 Wt. Images of Axial, Coronal & Sagittal sections.
FINDINGS:
MRI :
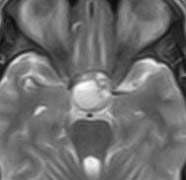
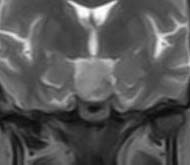
3.0 cm well defined smooth marginated
iso intense lesion on T1 and slightly hyper intense lesion with
fluid fluid levels which are hyper intense on T1 and
mixed intense on T2 noted in the sella and supra sellar
regions. Lesion is figure of eight in the coronal sections &
displacing abutting the optic chiasm Sell is widened.
DIAGNOSIS:
Pituitary macro adenoma with hemorrhage and abutting the optic
chiasm
Differential Diagnosis :
Pituitary hyperplasia
-
25-50% of
females 18-35 years have upwardly convex pituitary
Usually <10 mm
unless pregnant, lactating
Homogenous
enhancement
Normal
pituitary function
-
Can occur with
end-organ failure (e.g. ovarian, thyroid)
-
If prepubescent
female or young male has "adenoma-looking" pituitary, do endocrine
workup.
Aneurysm
-
Usually
eccentric, not directly suprasellar
-
Pituitary gland
visible, identified separate from mass
-
"Flow void"
common on MR
-
Ca++ more
common (rare in adenoma)
Meningioma (diaphragma sellae)
-
Pituitary gland
visible, can be identified separate from mass
-
Diaphragma
sellae identifiable as thin, dark line between mass (above) and
pituitary gland (below)
-
Dural
thickening more extensive than with adenoma
Metastasis
-
Diffuse skull
base invasion by adenoma may mimic more ominous disease
-
Occasionally
can see systemic metastases to stalk, pituitary gland.
Lymphocytic hypophysitis
-
Can mimic
adenoma clinically, on imaging studies
-
Most common in
peripartum female
Craniopharyngioma
-
Ca++, cysts
more common
-
Children >
adults
-
Rim/nodular >
solid enhancement
TIPS
-
Aggressive
adenomas extend inferiorly, invade sphenoid, may destroy upper
clivus
-
Giant adenoma
=> 4 cm in diameter. Prolactin levels are often > 1000 ng/ml
-
No matter how
aggressive/invasive adenoma looks, Pituitary tumors are almost never
malignant
REFERENCE : Osborn, Diagnostic Imaging,
Brain 1st edition, 2004.
SUBMITTED
BY: Academic division, 'MA' Advanced Diagnostic & Research Centre,
Guntur, AP. INDIA.
DR. M.ADINARAYANA RAO. MD.
DR. G.GOWRI SEKHAR . DNB.,DMRD.
DR. D. PRASAD REDDY. DMRD.
DR. Ch.SIVARAMA KRISHNA. DM(Neurology)
|